From 'Slipped Disc', Injections and Fear
— Back to Living, Freedom,
and the Forgotten Back.
Telehealth management of persistent disabling low back pain. Seven sessions. Three and a half months. The full story, the evidence, and three clinical tools you can use tomorrow.
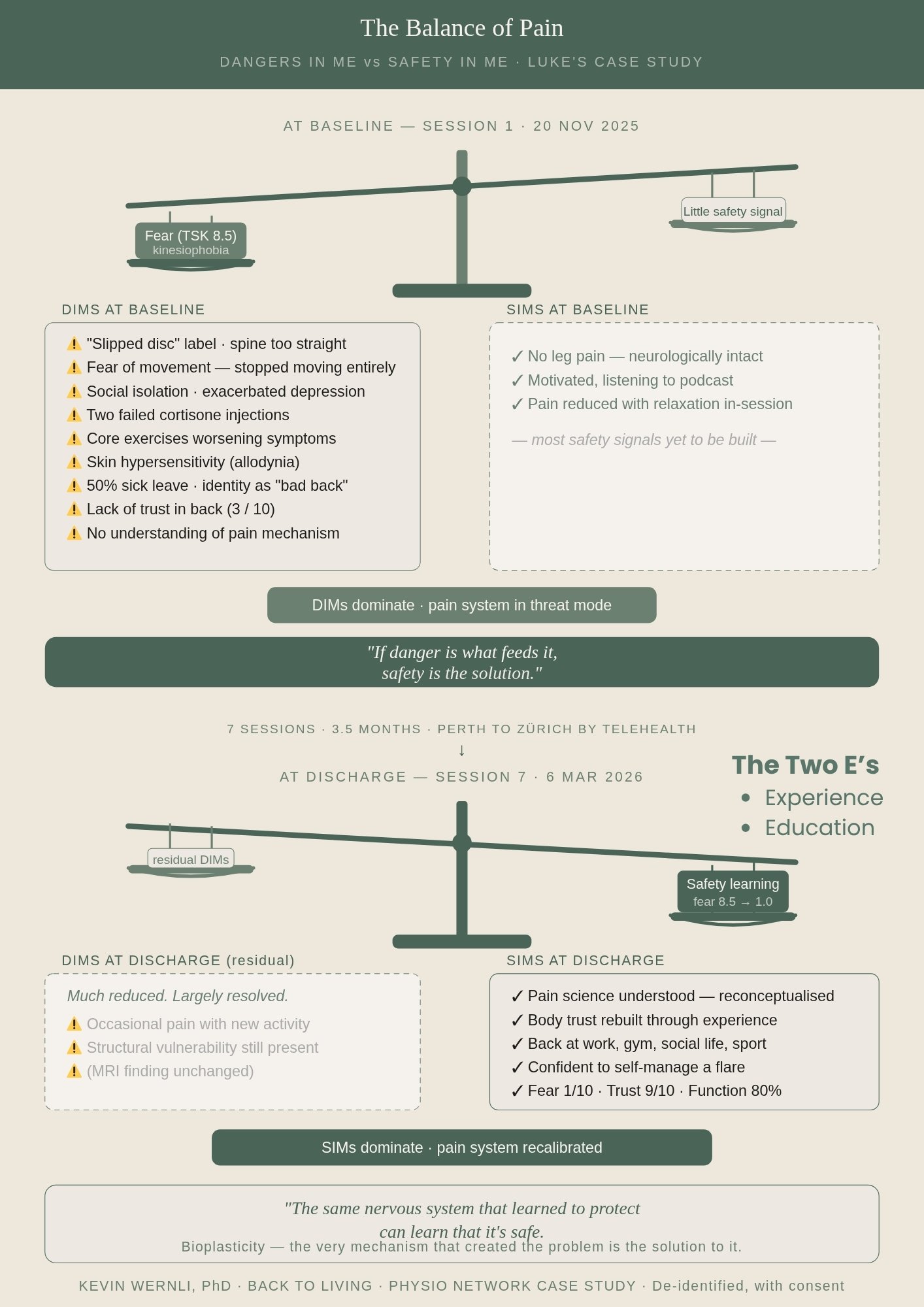
Luke (not his real name) is a 29-year-old product manager from Switzerland. After 7–8 months of back pain, two cortisone injections, multiple physiotherapy courses, and 50% sick leave, he came to telehealth with one question: will I ever get better? This page contains the full story — session-by-session highlights, key pain science concepts, three clinical tools, a companion podcast episode, and supporting videos and infographics.
The key ideas from this case — drawn from cognitive functional therapy, pain reprocessing therapy, and contemporary pain neuroscience.
Three things you can take into your clinic tomorrow — the specific language, questions, and frameworks used with Luke.
- Ask the patient to perform a provocative movement (sit-to-stand works well) in their usual braced, protected way. Note their pain rating.
- Ask them to relax their belly, breathe out, soften their shoulders, and repeat — without bracing.
- Note the difference. Let them feel it first. Don't explain yet.
- Then ask: "What does that tell you about what's driving the pain?"
- "What does your body do first when you prepare to move?" — surfaces the bracing, breath-holding, and tension they're not consciously aware of.
- "What happens to the pain if you relax and breathe before you do it?" — generates the experiment.
- "What does that tell you about what's driving the pain?" — shifts the locus of learning to the patient, not the clinician.
- Ask the patient to identify and make a list of their most feared, avoided, or provocative movements, postures, and tasks — including things they think are bad, or have been told are bad.
- Ask the patient to rank them: most threatening at the top, least threatening at the bottom.
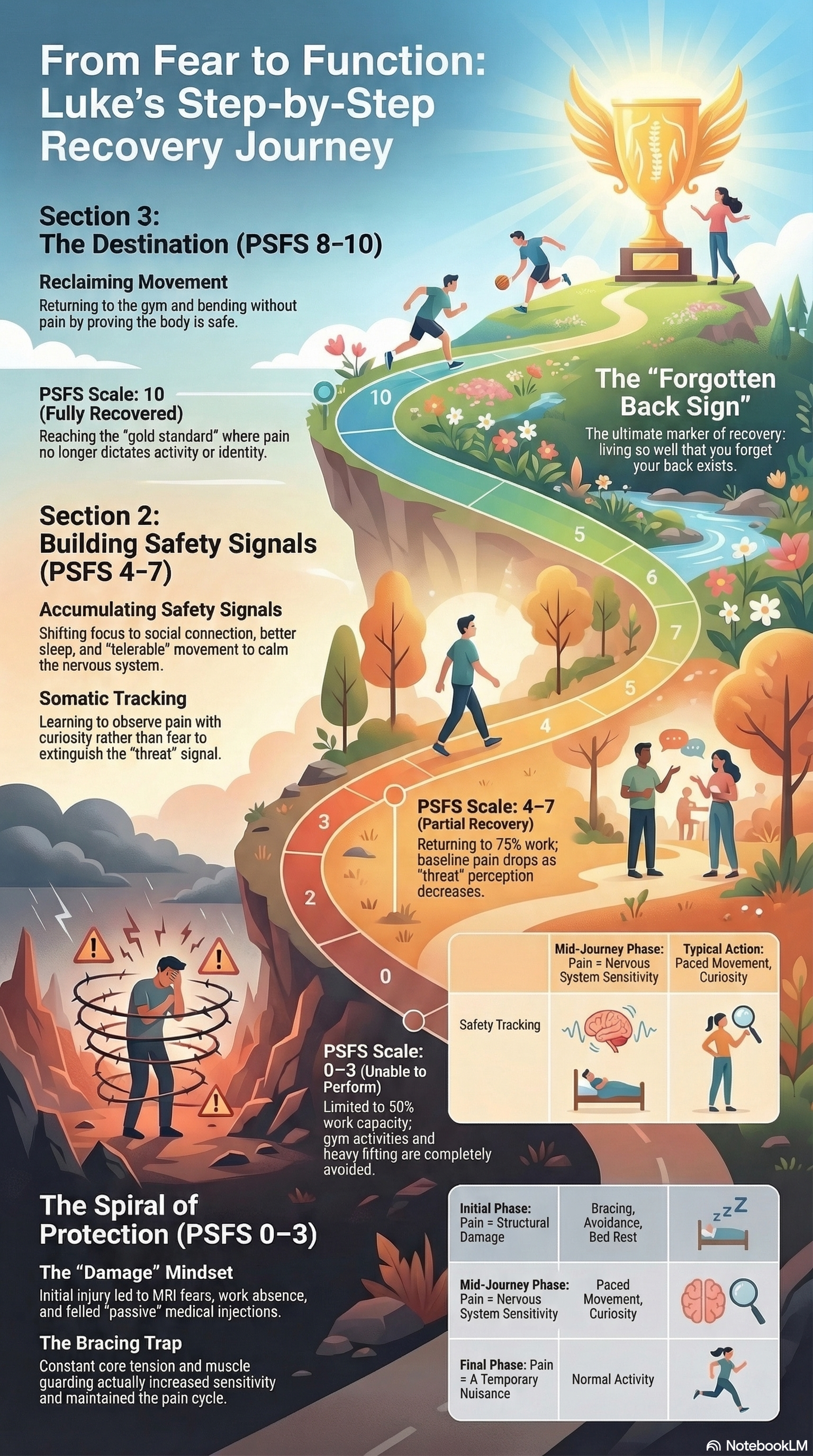
- Start at the bottom — or wherever the patient feels 80–90% confident they will be fine — and design the smallest possible behavioural experiment. Encourage the patient to perform the task with body regulation: calm, mindfulness, relaxation, and breathing. The goal is to increase signals of safety and reduce unhelpful overprotective bracing behaviours. Luke's first experiment was a cup, not a barbell.
- Build safety evidence upward. Each win reduces the threat value of the task and builds experiential evidence of safety. The nervous system learns it's safe and no longer produces overprotective perceived danger pain — a mechanism called safety learning.
- Consistency and repetition of even boring, sub-maximal tasks — without feared or unintended consequences — is what drives nervous system and pain system recalibration.
- Gradually climb the threat ladder and add further challenging contexts: stressful environments, distraction, external loads, unpredictable situations.
- The outcome of whether the task is less (or more) painful actually doesn't matter that much. The reduction of threat — how fearful or worrying the activity is — matters more, because pain is a downstream consequence of sensation combined with meaning (fear, attention, danger).
Sensation + Meaning (attention, fear, worry, threat) = Pain / conscious experience
Sensation + Nothing (no meaning, no significance) = Nothing — the nervous system deprioritises it and it drops into the subconscious.
Example: You can probably feel your foot on the floor right now — because I just mentioned it (meaning/attention). But before I mentioned it, you weren't aware of the sensation at all, even though your sensory receptors were still firing.
- "Are you doing everything you want to be doing?"
- "Are you avoiding anything — even implicitly?"
- "Are you confident to manage a pain flare if and when it comes?"
A companion podcast episode exploring Luke's recovery story — generated from the session transcripts using NotebookLM. It covers the key turning points, clinical reasoning, and pain science concepts from this case in a conversational format.
Short videos exploring the pain science concepts from this case — for clinicians wanting a visual walkthrough and for patients looking to understand their own pain.
Kent P et al. Cognitive functional therapy vs usual care (RESTORE). Lancet 2023.
Hancock M et al. RESTORE 3-year follow-up. Lancet Rheumatology 2025.
Ashar YK et al. Pain Reprocessing Therapy RCT. JAMA Psychiatry 2022.
Wernli K et al. Protection to non-protection. European Journal of Pain 2022.
Leake HB et al. What patients value learning about pain. PAIN 2021.
Kent P et al. Cognitive functional therapy vs usual care (RESTORE). Lancet 2023.
Hancock M et al. RESTORE 3-year follow-up. Lancet Rheumatology 2025.
Ashar YK et al. Pain Reprocessing Therapy RCT. JAMA Psychiatry 2022.
Wernli K et al. Protection to non-protection. European Journal of Pain 2022.
Leake HB et al. What patients value learning about pain. PAIN 2021.
Video’s based off the session transcripts
The Threat to Safety Spectrum
The Myth of the Broken Back
An AI Generated Podcast from the Session Transcripts
An AI developed podcast based on the audio recordings/transcripts of Luke’s 7 telehealth sessions
The Threat to Safety Spectrum